Disclaimer: This article is for educational purposes only and does not constitute medical advice. Always consult a healthcare professional before starting any treatment.
The rapid rise of GLP-1 receptor agonists like semaglutide (Ozempic/Wegovy) and tirzepatide (Mounjaro/Zepbound) has revolutionized the management of type 2 diabetes and obesity. However, as millions of patients in the USA and globally reach their weight loss goals, a new clinical phenomenon has emerged: “Ozempic Face.”
Characterized by a gaunt, aged appearance, sunken eyes, and sagging skin, “Ozempic Face” represents a complex interplay of rapid fat loss, altered cellular signaling, and compromised dermal structure. Recent research reveals this phenomenon extends beyond simple volume depletion—it involves direct effects on adipose-derived stem cells (ADSCs) and dermal fibroblasts that accelerate facial aging even beyond what weight loss alone would cause.
Clinical Case Observation: Managing Volume Loss in a 52-Year-Old Patient
“Consider a recent case involving a 52-year-old male patient on a 1.0 mg weekly dose of semaglutide for 36 weeks.
After a successful 10 kg weight loss, the patient presented with significant midface deflation and periorbital hollowing—the classic ‘Ozempic Face’ phenotype.
While many patients immediately seek dermal fillers like Juvederm or Restylane, this case highlights the importance of structural priming first.”
The Clinical Intervention:
Rather than immediate fillers, the strategy focused on a ‘Physiological Recovery’ phase.
This included increasing daily protein to 1.5g/kg and introducing a polynucleotide-based biostimulator to support the dermal matrix.
Within 8 weeks, imaging showed improved skin texture and a natural restoration of the ‘Ogee curve’ of the cheek, proving that supporting the dermal white adipose tissue (DWAT) is just as important as the weight loss itself.
Clinical Significance:
The American Academy of Facial Plastic and Reconstructive Surgery reported a 50% increase in facial fat grafting procedures in 2024, driven by the Ozempic face.
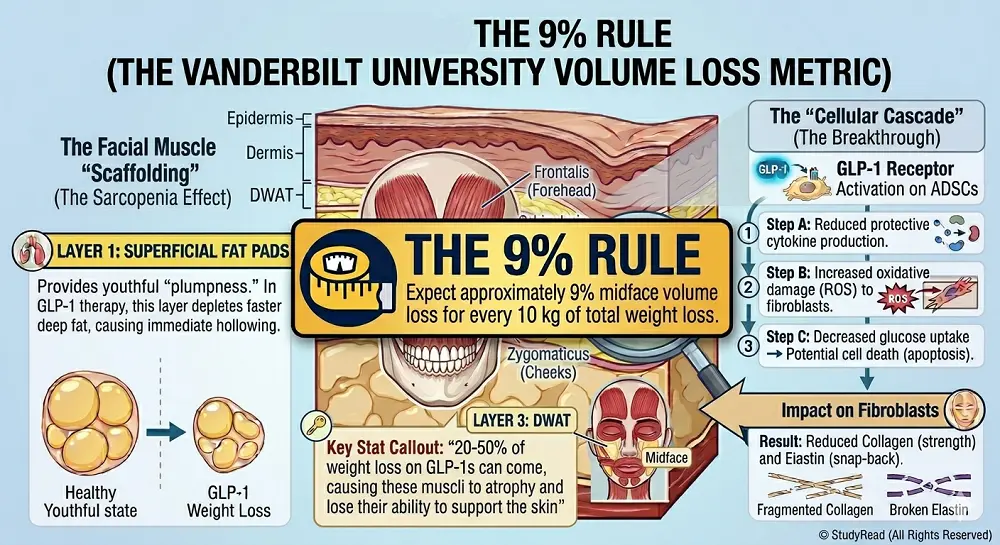
A 2025 Vanderbilt University study quantified approximately 9% midface volume loss for every 10 kg of total weight loss—a critical metric for patient counseling.
While lifestyle changes are essential, many US patients now use preventative medical aesthetics to prevent Ozempic face before the 9% volume loss threshold is reached.
The Pathophysiology: Why the Face Ages Rapidly on GLP-1s
Understanding “Ozempic Face” requires examining both systemic effects on weight loss and direct cellular mechanisms. The phenomenon is not merely cosmetic—it reflects fundamental alterations in adipose-derived stem cell function, dermal fibroblast activity, hormonal signaling, and collagen metabolism.
1. Selective Adipose Depletion and DWAT Loss
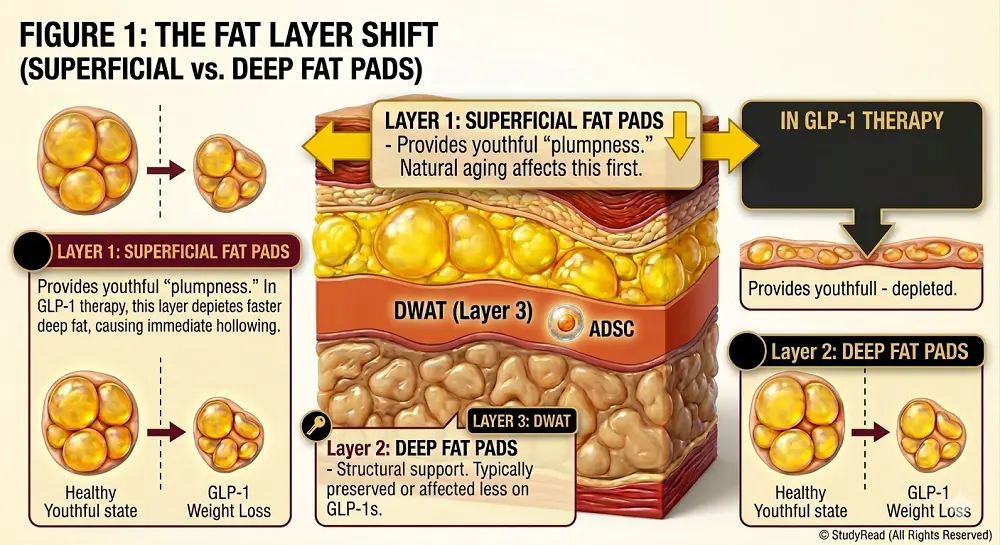
Facial Fat Architecture: The face contains three distinct adipose layers critical to youthful appearance:
- Superficial Fat Pads – Provide the “plump,” youthful contour of the face
- Deep Fat Pads – Provide structural support and maintain facial proportions
- Dermal White Adipose Tissue (DWAT) – A specialized layer that produces collagen-stimulating factors and maintains dermal thickness
Critical Research Finding:
In patients taking GLP-1 medications, most volume loss occurs in the superficial fat compartment—the opposite pattern of normal aging, where deep fat compartments typically deplete first.
This creates a distinctly “hollowed” appearance rather than the gradual facial thinning seen with natural aging.
During rapid weight loss induced by GLP-1 therapy, superficial fat pads often deplete faster than the skin can adapt through normal remodeling.
Additionally, aged skin is characterized by decreased DWAT volume, leading to reduced collagen production and increased metalloproteinase-1 activity (an enzyme that degrades collagen).
2. Facial Muscle Atrophy (Sarcopenia)
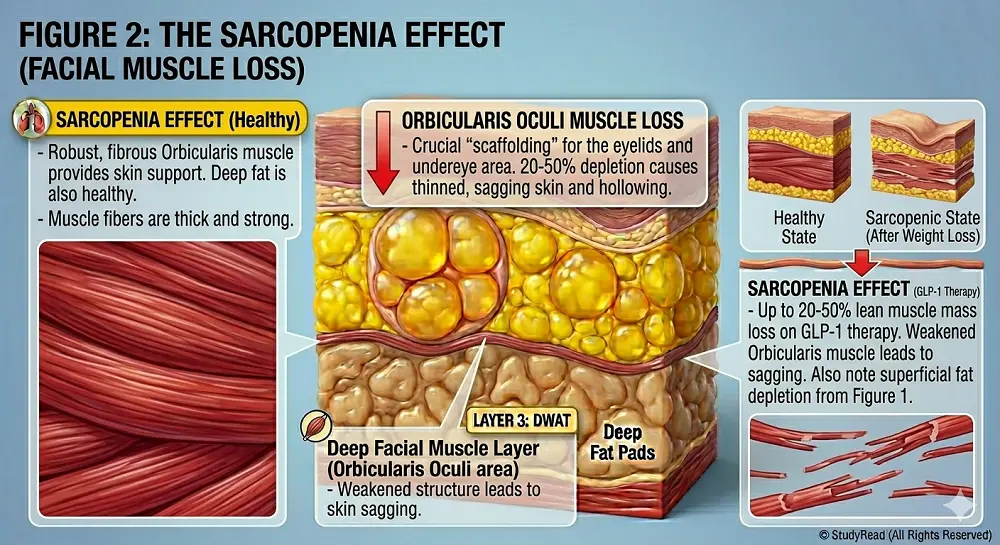
- Research indicates that 20-50% of the total weight loss during GLP-1 therapy results from catabolism of lean mass (skeletal muscles, connective tissue), including the delicate muscles of facial expression.
- These small but crucial muscles, such as the orbicularis oculi (around the eyes), zygomaticus (cheeks), and frontalis (forehead), provide underlying support for facial contour.
When facial muscles atrophy, the overlying skin has less structural support, contributing to the hollow, aged appearance characteristic of “Ozempic Face.”
3. Direct Cellular Mechanisms: Beyond Simple Fat Loss
2025-2026 Breakthrough Research:
- Recent studies reveal that GLP-1 receptor agonists don’t just cause weight loss.
- They directly affect the cells responsible for skin health and regeneration.
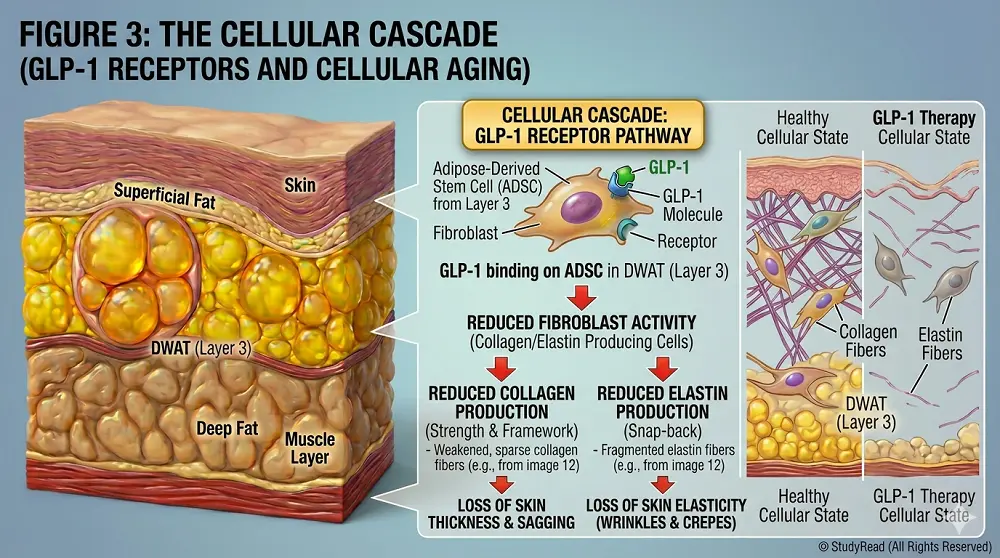
GLP-1 Receptors on Adipose-Derived Stem Cells (ADSCs):
GLP-1 receptors exist directly on ADSCs and dermal fibroblasts. When activated by medications, these receptors trigger several detrimental cascades:
- Reduced protective cytokine production from ADSCs, promoting reactive oxygen species (ROS) production and oxidative damage to fibroblasts
- Decreased glucose uptake in ADSCs → reduced ATP production → potential cell death (apoptosis)
- Reduced estrogen production from dermal white adipose tissue (DWAT) → decreased fibroblast stimulation → lower collagen synthesis
- Impaired cellular metabolism → accelerated aging of the dermal support structure
Clinical Implication: This means “Ozempic Face” is not purely a volume problem that can be solved with fillers—it represents fundamental changes in skin cell function that require targeted nutritional and therapeutic interventions.
4. Compromised Dermal Fibroblast Function
Rapid weight loss is often accompanied by inadequate protein intake and micronutrient absorption. This nutritional deficit, combined with direct GLP-1R activation on fibroblasts, leads to:
- Decreased collagen synthesis – The structural protein that gives skin its strength
- Reduced elastin production – The protein responsible for the skin’s “snap-back” quality
- Impaired extracellular matrix (ECM) remodeling – Preventing the skin from “shrinking” to fit new facial contours
Without adequate collagen and elastin, skin loses its structural integrity and elasticity (recoil), making facial volume loss dramatically more apparent.
5. Age-Related Vulnerability
- Baseline collagen decline: After age 30, collagen production naturally declines at approximately 1% per year.
- After menopause, women experience an accelerated drop, losing up to 30% of dermal collagen in the first five years post-menopause.
- This means postmenopausal women starting GLP-1 therapy face a “double hit“-already compromised collagen production combined with medication-induced cellular changes.
- This population requires especially aggressive preventive strategies.
Who Is Most at Risk for “Ozempic Face”?
Not all patients on GLP-1 therapy will develop significant facial aging. But, people with certain risk factors are more prone to develop it, like:
- Age >40 years – Baseline collagen decline makes facial tissues less resilient.
- Postmenopausal women – Already experiencing 30% collagen loss in the first 5 years post-menopause.
- Rapid weight loss rate >1.5 kg/week – Skin cannot remodel fast enough.
- Higher starting doses of GLP-1RAs – More aggressive appetite suppression and cellular effects.
- Pre-existing photoaging – UV damage has already degraded your facial collagen reserves.
- Poor baseline nutrition – Inadequate protein or micronutrient intake before starting the therapy.
- Genetic factors affecting skin elasticity – Family history of thin skin or poor wound healing.
- Smoking history – Nicotine intake significantly impairs microcirculation and collagen synthesis.
12 Evidence-Based Strategies to Prevent “Ozempic Face.”
To prevent the aged appearance associated with GLP-1 therapy, one must try to balance systemic lipolysis with dermal structural integrity and cellular health.
The following strategies are based on pharmacology, nutrition science, and the latest dermatological research.
1. Prioritize High-Quality Protein Intake
Target:
- 1.2-1.5g of protein per kilogram of ideal body weight (not current weight for obese patients).
- For a 70kg goal weight patient, this equals 84-105g of protein daily.
Why: A rapid weight loss causes facial muscle loss (sarcopenia), particularly the delicate muscles of facial expression.
- High-quality protein intake provides amino acids like proline, glycine, and hydroxyproline, which are building blocks of collagen.
- Adequate protein also preserves facial muscle mass, maintaining underlying structural support.
Best sources: Eggs, Greek yogurt, lean poultry, fish (especially salmon), legumes, etc.
2. The “Slow and Steady” Dose Titration Rule
Comparison: Normal vs. Rapid Weight Loss (Facial Impact)
| Feature | Gradual Weight Loss (0.5kg/week) | Rapid GLP-1 Weight Loss (>1.5kg/week) |
| Skin Elasticity | Skin usually adapts to volume loss through ECM remodeling | High risk of skin laxity (sagging); ECM cannot remodel quickly enough |
| Fat Pad Preservation | Balanced depletion across the body; deep fat is preferentially lost | Accelerated depletion of superficial facial fat; hollow appearance |
| ADSC Function | Normal stem cell activity supports tissue regeneration | Direct GLP-1R activation impairs ADSC protective functions |
| Fibroblast Activity | Usually maintained with steady nutrition and hormonal support | Potential ‘starvation’ of collagen cofactors; reduced estrogen signaling |
| Facial Muscle Mass | Preserved with adequate protein; maintains facial support | 20-50% of weight loss from lean mass; facial muscle atrophy |
| Appearance | Healthy ‘glow’ and natural facial definition | Gaunt, ‘shadowed’ under-eye and cheek areas; aged appearance |
Pharmacological Principle:
- The risk of skin laxity increases exponentially with the speed of weight loss. i.e., faster weight loss leads to more rapid facial muscle loss.
- So, a slower weight-loss rate of 0.5-1.0 kg per week gives the skin’s extracellular matrix (ECM) sufficient time to remodel and “shrink” to fit new facial contours.
Best practice: Patients should work with their healthcare providers to stay on the lowest effective dose for as long as possible.
- Resist the temptation to quickly escalate to maximum doses.
- Slower titration produces more sustainable results with better facial aesthetics.
Key Metric: Expect approximately 9% midface volume loss for every 10 kg of total weight loss. This helps set realistic expectations and guides dose adjustments.
3. Supplement with Collagen Cofactors
Despite the intake of collagen peptide supplements, the body needs specific micronutrient cofactors to synthesize functional collagen. So, ensure adequate intake of:
- Vitamin C (1000mg daily) – Essential for hydroxylation of procollagen; without it, collagen cannot form its triple helix structure.
- Zinc (15-30mg daily) & Copper (1-2mg daily) – Necessary for cross-linking elastin fibers and collagen maturation.
- Iron (8-18mg daily) – Required for oxygenation of dermal tissues and collagen hydroxylase enzymes.
- Silica (10-40mg daily) – Promotes collagen synthesis and skin elasticity
- Vitamin A (retinol) – Stimulates fibroblast activity and collagen gene expression
4. Focus on Intracellular Hydration
GLP-1 medications can shift fluid balance, and dehydrated skin appears thinner and more wrinkled. Beyond drinking adequate water (2-3 liters daily), patients must ensure proper electrolyte balance to maintain intracellular hydration:
- Sodium – Maintains extracellular fluid volume
- Potassium – Critical for intracellular water retention and cell turgor
- Magnesium – Supports cellular energy production and protein synthesis
Well-hydrated cells maintain facial “plumpness” at the cellular level, partially offsetting volume loss from fat depletion.
5. Implement “Skin-First” Topical Skincare
While volume loss occurs in deep fat compartments, medical-grade topical treatments can improve surface elasticity and epidermal thickness:
- Prescription Retinoids (tretinoin 0.025-0.1%) – Increase cell turnover, thicken the epidermis, and stimulate dermal collagen production. Start low concentration to avoid irritation.
- Topical Vitamin C (L-ascorbic acid 10-20%) – Powerful antioxidant that boosts collagen synthesis and protects against UV damage
- Hyaluronic Acid Serums – Acts as a humectant to pull moisture into the skin surface, temporarily reducing the appearance of fine lines
- Peptide Complexes – Signal peptides (e.g., Matrixyl, copper peptides) may stimulate fibroblast activity
6. Resistance Training for Growth Hormone Stimulation
High-intensity resistance training isn’t just for building body muscle-it stimulates natural production of Growth Hormone (GH) and Insulin-Like Growth Factor-1 (IGF-1), both of which play crucial roles in:
- Preserving facial muscle mass – Prevents atrophy of small facial expression muscles
- Skin thickness and cellular repair – GH stimulates fibroblast proliferation and collagen synthesis
- Lean mass preservation – Counteracts the 20-50% lean mass loss typical of GLP-1 weight loss
Recommendation: 3-4 sessions per week of compound movements (squats, deadlifts, rows, presses) with progressive overload.
7. Address “Dermal Starvation” with Healthy Fats
Because GLP-1 medications suppress appetite, many patients inadvertently tend to eliminate healthy dietary fats.
This creates “dermal starvation,” and the skin’s lipid barrier becomes compromised, leading to:
- Transepidermal water loss (TEWL) – Skin becomes dry and brittle
- Impaired fat-soluble vitamin absorption – Vitamins A, D, E, and K are critical for skin health
- Reduced cellular membrane integrity – Every cell needs lipids for proper function
Essential healthy fats: Patients should consume Omega-3 fatty acids (EPA/DHA from fish oil or algae), avocados, extra virgin olive oil, nuts (especially walnuts and almonds), and seeds (chia and flax). One must aim for 20-30% of daily calories from healthy fats.
8. Facial Massage and Microcirculation Enhancement
Stimulating blood flow to facial tissues helps deliver nutrients to the dermal layer ADSCs and promotes the removal of metabolic waste products. One must try
- Manual lymphatic drainage massage – Reduces facial edema and improves nutrient delivery
- Gua Sha or jade rolling – Traditional techniques promote circulation
- Facial exercises – May help maintain facial muscle tone, though evidence is limited.
Increased microcirculation may also partially counteract the reduced cellular metabolism caused by direct GLP-1R activation on dermal cells.
9. Effective Sun Protection
- UV radiation from the sun breaks down existing collagen by activating the enzyme matrix metalloproteinases (MMPs).
- When a patient is already losing facial volume due to weight loss and has impaired collagen synthesis from GLP-1 cellular effects, they cannot afford additional UV-induced collagen degradation.
Protocol: A Daily broad-spectrum SPF 30+ (SPF 50+ preferred), and reapply every 2 hours during sun exposure.
- Combine with antioxidant serums (vitamin C, E, ferulic acid) for additional photoprotection.
10. Consider Professional “Biostimulators” Over Traditional Fillers
For patients already experiencing significant facial volume loss, the treatment approach should shift toward biostimulation rather than simple volume replacement:
- Sculptra (poly-L-lactic acid) – Stimulates endogenous collagen production over 3-6 months; provides gradual, natural-looking volume restoration
- Radiesse (calcium hydroxylapatite) – Immediate structural support with sustained collagen stimulation
- Platelet-Rich Plasma (PRP) / PRF injections – Uses the patient’s own growth factors to stimulate tissue regeneration
- Microneedling with PRP – Creates controlled micro-injuries that trigger a healing response and collagen production
Critical Timing: Patients should ideally wait at least 6 months after achieving a stable weight before considering surgical interventions or major filler treatments, as peak weight loss typically occurs at 52 weeks after starting GLP-1 receptor agonists. Premature intervention may require additional correction as weight continues to change.
11. Support Estrogen-Dependent Collagen Pathways
Given that GLP-1R activation reduces estrogen production from DWAT, postmenopausal women on GLP-1 therapy face a particularly severe collagen deficit.
Consider:
- Topical estrogen therapy – May support dermal fibroblast activity (requires physician consultation)
- Phytoestrogens – Soy isoflavones, red clover, may provide weak estrogen-receptor activation
- Hormone replacement therapy (HRT) – For appropriate candidates, systemic HRT preserves skin thickness and collagen content
12. Monitor and Document Facial Changes
Proactive monitoring allows early intervention before changes become severe: So one needs to check
- Monthly standardized facial photographs – Same lighting, angles, and facial expressions to track changes
- Skin elasticity testing (pinch test) – Pinch cheek skin and note how quickly it rebounds
- Weight loss rate tracking – Weekly weigh-ins to ensure rate stays within 0.5-1.0 kg/week
- Nutritional intake logging – Verify adequate protein, micronutrients, and healthy fats
🚩 Red Flags: When to Slow Down Your GLP-1 Dose
Contact your healthcare provider if you notice:
- Weight loss >1.5 kg per week for more than 2 consecutive weeks
- Rapid emergence of under-eye hollowing or cheek gauntness
- Skin that doesn’t bounce back after pinching (>3 seconds to return)
- Inability to meet protein targets due to severe appetite suppression
- Hair loss, brittle nails, or other signs of protein/micronutrient deficiency
- Excessive fatigue or muscle weakness
- Development of new, deep facial wrinkles within weeks
Early recognition and dose adjustment can prevent irreversible changes.
Remember: The goal is sustainable, healthy weight loss with facial aesthetics preserved—not maximum speed of weight reduction.
Conclusion: Balancing Weight Loss with Facial Preservation
The emergence of “Ozempic Face” represents a significant clinical challenge, but it is largely preventable through proactive, evidence-based interventions. The key is understanding that this phenomenon is not merely cosmetic—it reflects fundamental alterations in adipose-derived stem cell function, dermal fibroblast activity, hormonal signaling, and collagen metabolism.
By implementing the 12 strategies outlined above—particularly slow titration, aggressive protein intake, micronutrient supplementation, resistance training, and appropriate skin protection—patients can achieve their weight loss goals while maintaining a healthy, youthful facial appearance.
For healthcare providers, patient education is paramount. Set realistic expectations about midface volume loss (≈9% per 10 kg), establish regular monitoring protocols, and maintain open communication about facial changes. Remember that successful GLP-1 therapy isn’t just about the number on the scale—it’s about comprehensive metabolic health with preserved quality of life and self-image.
The convergence of pharmacology, nutrition, dermatology, and aesthetic medicine offers powerful tools to prevent “Ozempic Face.” With proper knowledge and proactive management, patients can transform their health without sacrificing their facial aesthetics.
Key References and Further Reading
- American Academy of Facial Plastic and Reconstructive Surgery: 2024 procedural trends report on facial fat grafting
- Vanderbilt University Medical Center (2025): Quantitative analysis of midface volume loss with GLP-1 receptor agonist therapy
- Journal of Dermatological Science: GLP-1 receptor expression and function in adipose-derived stem cells and their role in dermal aging (2025-2026)
- Clinical studies on lean mass preservation during GLP-1 therapy: Role of protein supplementation and resistance training
- Menopause and collagen metabolism: Accelerated dermal aging in the postmenopausal period
